Categories:

Defining and Delivering Maternal Health Equity: How We Can Achieve Culturally Relevant Healthcare for All Moms and Families
Jenné Johns, MPH is a leading health equity and quality improvement expert who has helped some of the nation’s largest payors transform their cultures to be more sensitive to the needs of the medically vulnerable while closing gaps based on race and ethnicity. She is the author of, “Once Upon A Preemie,’ an inspirational book based on her life-changing experience of nurturing her micro-preemie son out of the NICU. She also has launched Once Upon a Preemie Academy, a first of its kind training for perinatal and neonatal professionals, focused on health equity, racial equity and implicit bias . Wildflower recently interviewed Jenné to discuss health equity challenges within the maternal health space.
Can you quantify the current level of inequity we see in maternal health outcomes in the U.S.?
While the United States now has better maternal mortality data, African American women die at a rate three times higher than their counterparts according to the Centers for Disease Control and Prevention. Recent March of Dimes reports suggest that African American women have a premature birth rate that is 49 percent higher, and African American babies die prematurely at a far greater rate. Black babies are more than twice as likely to die before their first birthday. We need to find better solutions for communities who have historically and systematically experienced less than optimal health outcomes based on systematic racism.
In many cases, people use the terms health equity and health equality interchangeably. In reality, that’s not accurate. What is the difference?
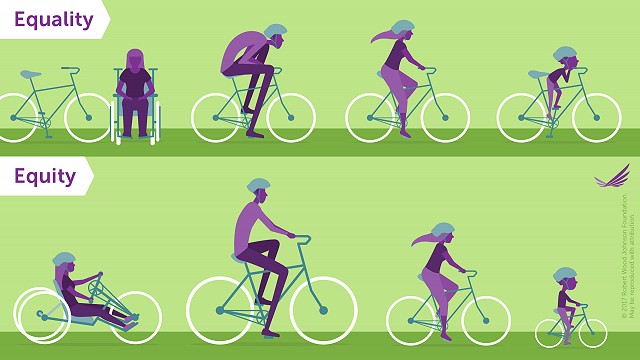
There is a great graphic used by the Robert Wood Johnson Foundation to illustrate the difference between equality and equity. Let’s say there are several individuals who need to access a bicycle to reach a destination. Equality ensures that everyone gets a bike. With equality, you don’t consider personal differences in terms of their ability to use the bike and whether the bike needs to be altered in some way to better assist them. With equity, everyone’s bike would be customized to meet their individual needs, such as height, weight, and disability status.
Specifically in the maternity space, equality says everyone gets access to healthcare. Equity goes a step further. It says we will help women receive care that meets their specific cultural, linguistic and risk-based needs.
Where should we start if we want to improve the system so that it delivers equitable care to all mothers?
First, we need routine and continuous training and education. Our entire clinical community must participate in learning about cultural competency, health and racial equity, and we need to check our own biases. To see improved practices, we have to change hearts, minds and attitudes.
We also must do a better job of listening to the needs of women. The concerns expressed by African American women are not adequately captured and responded to in our system today. The system doesn’t really track and quantify patient voice, or patient lived experience. Clinicians can create opportunities for positive change by improving their listening skills.
We should address individual biases. When we uncover bias, it’s our duty to check it at the door as an individual, team and organization wide. We need bias-free cultures where care is delivered consistently to women regardless of their race, ethnicity, income and education levels, or insurance status.
You believe digital health can play a role in increasing equity as well. Tell us more about that.
Digital health is revolutionary in this space. There’s so much innovation and creativity waiting to happen. But we have not yet fully tapped into it. When a women has access to technology, it offers them an opportunity to find what has been missing.. But we have to make sure our tools are geared to meet the unique needs of each woman, ranging from messaging to imagery to language to cultural preferences. The more we address those differences, the more we can create better connections to clinical supports and start to close some of the gaps in care based on racial disparities.
We must also create a culture of technology. In maternal health, particularly in African American communities, healthcare is very high touch. We have to get these communities more comfortable relying on technology for better access and education and as a more effective and efficient method of communicating with providers.
Bottom line, we have a unique opportunity to use technology to provide education for pregnant women, and for the provider and clinical community, to look for different signs and symptoms that can help prevent fatalities and advocating for women to get them the help they need, when they need it. Going back to our bicycle analogy, digital solutions can enable personalization that is sensitive and specific to meet individual needs.
Wildflower is really a pioneer, and a great example of using technology to empower real-time support for women. I also like that Wildflower is committed to developing solutions that are culturally sensitive and equitable. By deploying these culturally appropriate solutions they also are breaking down silos to help providers and payers work together to address inequities in maternal care.
How did you come to focus on health equity in the maternity space?
During my tenure with one of the nation’s largest commercial insurers, I was responsible for organizational transformational strategies to reduce racial and ethnic health disparities. I spent ample time leading strategic planning at the enterprise and medical management department levels, as well as leading staff and provider annual health equity and cultural competency training. Unfortunately, while birthing my first son, who landed in the NICU, I did not see any of this cultural competency training or communications applied as I sat in the patient seat. We had a long 77 day journey through the NICU, and my health disparities and advocacy skills were tested daily. The NICU system lacked professional diversity, cultural sensitivity, and equitable distribution of resources for all families regardless of the location where they recevied care. We didn’t get access to the same resources made available to moms who were in the NICU at the health system’s higher income locations. We were not even offered education around basic health concerns such as the importance of human-fortified breast milk. Communication was lacking. I wasn’t satisfied with how the system responded to me as a woman of color, so I decided to do my part in making things better.
Do you think value-based care can support increases in equity?
I really think we need more joint training between payers and providers, as well as agreed upon accountability for improving health equity. This would include tracking and reporting on maternal birth outcomes by race, and where differences occur, developing culturally specific solutions to the issues at hand.
Tying performance to incentivize payments would also be powerful. I would love to see equity-centered goals as part of value-based agreements where both the payer and the provider are aligned to move the needle on maternity care. The environment is ripe for aligning maternity care and equity-centered goals based the growing momentum of value-based care.
What additional concerns do you have today?
One really big issue is that more black women are opting out of traditional hospital delivery. They don’t feel safe, so they are choosing in-home delivery options. We need women and babies to thrive and be healthy without the fear and stigma that something bad will happen if they seek care from a hospital system. We need better and trusted relationships between patients and providers so that all women feel safe enough to deliver their babies in whichever setting they desire.
About the Author
